

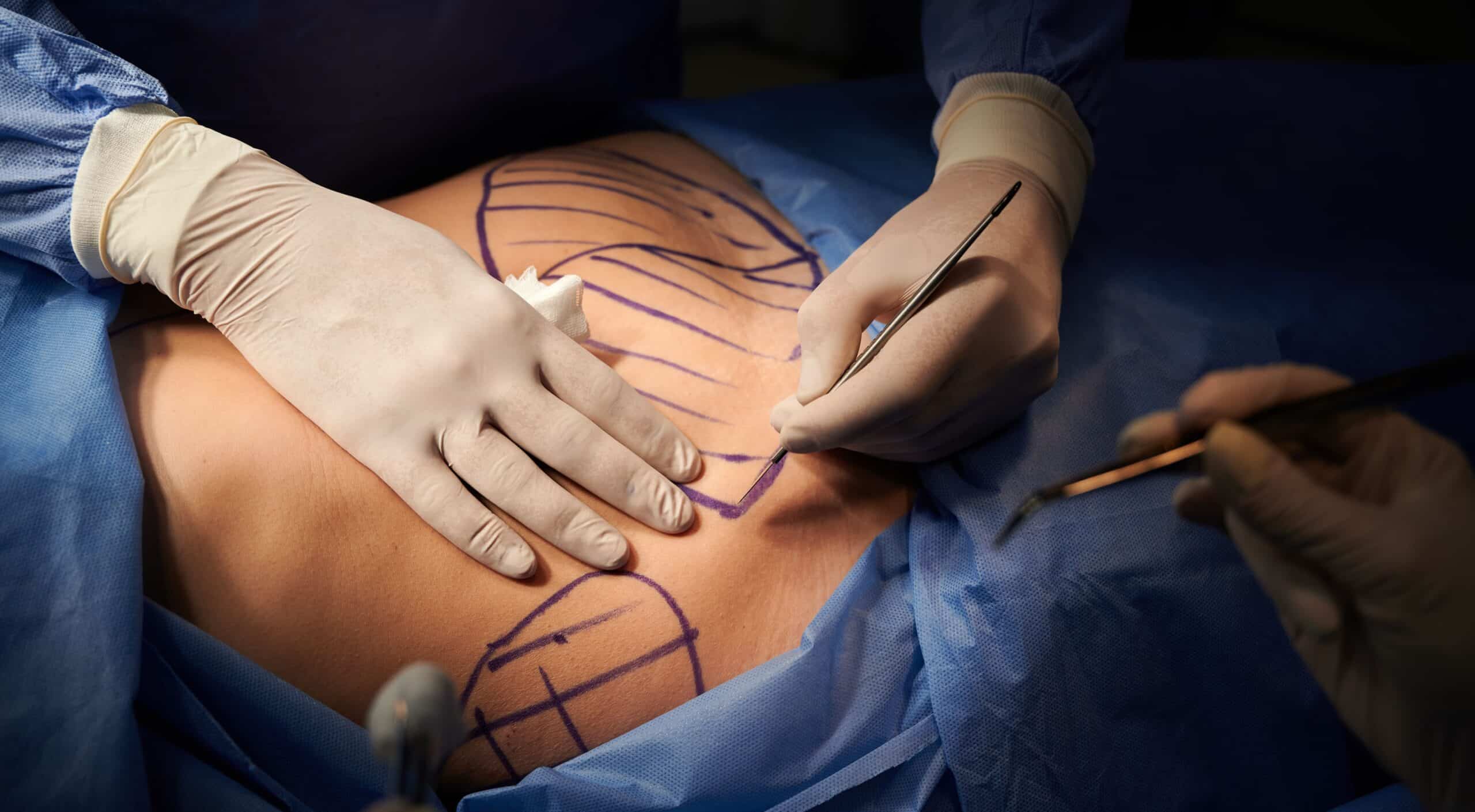
What is Post-Pregnancy Surgery?
Undergoing post-pregnancy surgery is something that requires serious consideration. The process can include surgical cosmetic procedures and therefore should be carried out by a qualified specialist surgeon – not just anyone with a cosmetic background. To help you understand what’s involved and the importance of choosing a specialist surgeon, we’ve updated this blog to bring you a new version of the post-pregnancy surgery guide.
Why consider Post-Pregnancy Surgery?
Pregnancy is a very natural process, as are normal vaginal deliveries. However, there are defined hormonal changes that occur from the time of conception and throughout the pregnancy, including changes before and during delivery all the way to the completion of lactation and breastfeeding.
It is only some months (3-6) after lactation has ceased that the pre-pregnancy hormone profile returns to normal levels. So, the changes to your body that result from this very natural process are significant and, in most cases, are permanent.
In discussing the concept of post-pregnancy surgery, two situations will arise.
The first outcome is your post-pregnancy weight (body fat content) is close to or equal to the pre-pregnancy weight (body fat content).
The second outcome is a large change in the post-pregnancy weight (body fat content), where the woman has noticeably increased her body fat content during her pregnancy.
The reason for this separation into two groups of women is important. The body changes are different and, therefore, the surgery will also be different.
Women with significant weight gain may undergo more complex operations but even more importantly, can require more operations on more body areas.
The Body After Pregnancy
The Abdomen
As your baby grows, your uterus enlarges, causing your abdomen to change. With the hormone changes that occur from the time of conception to the preparation for delivery and breastfeeding, oestrogen causes a degree of softening and laxity of the body’s tissues. This mainly impacts muscles, ligaments and tendons but also affects the skin.
With the uterus expanding, outward pressure starts to be exerted in the muscle layer of the abdomen. This results in a stretch of the abdominal muscles and, because of the effects of the hormone changes, the main ligament that joins the right and left sides of the muscles in the middle of the abdomen will also start to stretch.
It is also important to point out that the belly button (umbilicus) is situated within this abdominal ligament and is a natural scar. However, with the stretch of this central ligament, the belly button also stretches with the evolving pregnancy.
The result of this is the separation of the abdominal muscles but also, a number of women will develop an umbilical hernia. This manifests a protruding belly button (an “outy” instead of an “inny”).
The skin overstretches and the outcome is loose, lax skin with stretch marks that initially are red/pink but fade with time to become silvery-white.
If your baby is born by Caesarean section, then the scar together with the aforementioned skin changes results in the “overhang” of loose skin over the Caesarean section scar.
The Breasts
Regardless of their size, non-pregnant breasts consist mainly of fat with a much smaller breast gland component. With the hormonal changes, the breast gland component dramatically expands at the expense of the breast fat.
These are the early changes that ultimately result in milk production (lactation). The end result of these hormonal changes can be very enlarged breasts. After delivery and after breastfeeding, the hormonal profile returns to your pre-pregnancy state.
As a result, breast gland components return to their pre-pregnancy state. The breast fat component does not return as glands subside. Because the breast skin has expanded to accommodate the size increase of your breasts and your breasts’ loss of fat and volume, the skin expansion results in droop. Additionally, the hormonal changes have an impact on your skin overall. Pregnancy, childbirth and breastfeeding can also enlarge the pigmented skin around the nipple called the areola.
If you do consider post-pregnancy surgery, you need to wait until your baby is 6 months old. This ensures that the hormone profile will have returned to the pre-pregnancy state.
Vaginal Surgery
The next discussion point is much more personal and intimate. It is common during a vaginal delivery for a procedure called an episiotomy to be performed. This is a cut into the skin and tissues towards the back of the vaginal opening on the right side to prevent an uncontrolled vaginal tear from occurring.
Performing an episiotomy cut is precise and prevents unwanted tearing. In an uncontrolled situation, the tear can even extend backwards into the anal canal.
The episiotomy cut often involves the inner labia towards the back. Childbirth and multiple deliveries can lead to changes in the inner labia.
Post-pregnancy surgery procedures can include:
- Abdominoplasty
- Liposuction
- Caesarean section scar revision
- Mons pubis lift
- Breast augmentation
- Breast lift
- Breast reduction
- Labiaplasty
- Labial rejuvenation
- Vaginal canal rejuvenation
Cosmetic Procedures

Breast Surgeries
1. Breast Lift vs Breast Augmentation
At the consultation, I perform a series of measurements of the breasts, as well as the breast position on the chest wall. In addition, I assess the breast position in terms of certain landmarks that I assess and demonstrate at this consultation.
Here, it often becomes apparent that a breast lift surgery may in fact, NOT be necessary. In these cases, I offer and recommend a breast augmentation. The next discussion involves the size and shape of the implant that will give the best result possible for the individual woman in question.
If breast skin is loose and the breast base is wide, then, the implant will need to fill the breast “skin envelope.” This will be assessed at the consultation.
There are many options for this procedure. Unfortunately, this operation does not always result in a long-term solution. Breast droop is a natural phenomenon with time/age/gravity as well as weight gain and loss. Further pregnancies will adversely affect the breasts also. Droop is not preventable.
Some women are fortunate in that the breast supporting structures and ligaments delay droop. It is estimated that droop after a lift procedure can occur as early as 3 years after the surgery with the lesser “donut” lift or 5 or 7 years after the “classic” breast lift.
2. Breast Lift vs Breast Reduction
The boundaries between a breast lift and breast reduction are becoming increasingly blurred.
A breast reduction is a much more durable operation, often lasting a far longer time before droop sets in again—often in excess of 10 years! It is possible to perform this operation with implants as well. In this case, implants are more for shape than size.
Ultimately, this procedure can be performed with the removal of minimal breast gland tissue or a large amount of breast tissue, depending on the individual woman’s situation and what result she desires.
The incision (and therefore scarring pattern) is the same with classic mastopexy (lift) and a breast reduction: the so called ‘lollipop’ scar. This is a scar around the areolar (pigmented) skin and a vertical scar down the front of the breast into the crease under the breast. The old fashioned ‘anchor’ scar is rarely done today.
Abdominal Operations
1. Abdominoplasty Vs Liposuction
This is a far less complex scenario. There are only 2 options: namely an abdominoplasty or one form of liposuction. The crucial factor in deciding which option is best relates to the quality of the abdominal skin and the amount of excess fat present.
As discussed above, the normal body changes during pregnancy can result in over-stretched skin and overall abdominal laxity. In some cases liposuction is not an option; the only option is an abdominoplasty.
There are different ‘grades’ of abdominoplasty surgery, from minor removal of loose skin to major surgical procedures. Note that this operation is not designed to deal well with the upper abdomen.
If the amount of excess upper abdominal fat is significant, liposuction may be necessary for the upper abdomen. This liposuction is an integral part of the operation.
Standard liposuction involves a process of infiltrating the fat layer with saline (salt water) solution under pressure to water-log fat. A suction then removes this water-logged fat. There are now modern liposuction systems that include either ultrasound or laser energy to liquefy and emulsify fat prior to its removal.
These new systems allow a lower suction pressure to remove unwanted fat. The delivery of the ultrasound or laser accomplishes a significant part of the process. The result is that ultrasound or laser liposuction systems are far more accurate and will deliver overall better results than standard liposuction techniques.
Dr. Goldman is one of the very few specialists who have been trained in High Definition Liposuction, also known as ultrasound or laser liposculpture. There is one final difference between liposculpture and traditional liposuction. There is conclusive evidence that ultrasound and laser energy both stimulate the skin’s under-surface to make new collagen and elastin fibres.
This caused the skin to retract/contract down onto the newly formed fat layer. No other liposuction system has been shown to result in this degree of skin retraction.
The lowermost aspect of the abdomen is called the mons pubis. It is the junction or link between the stomach and the top of the vagina. The significance of this zone has very suddenly become an area of conversation for a large number of women due to the modern practices of pubic hair management.
The result of hair removal trends is that the skin of the mons pubis is now far more noticeable. After pregnancy, especially with significant weight gain, the mons pubis and the front aspect of the vagina (area just above the clitoral hood) descend to a lower level.
It is possible to perform specific operations to either flatten this area or to perform a lift of the mons pubis complex. Dr. Goldman evaluates this as part of the surgery, if specifically requested.
Vaginal Rejuvenation
Vaginal rejuvenation consists of labiaplasty, outer labia (labia majora) rejuvenation and vaginal canal lining rejuvenation. Vaginal rejuvenation is an elective part of the abdominoplasty surgery but yields substantial results.
1. Labiaplasty
There are several reasons why women may request this operation. The reasons are not always cosmetic (physical appearance) and include, for example, discomfort with activities and the wearing of certain items of clothing.
A labiaplasty is designed to result in the shortening of the overall length of the inner labia so that the “outers” will mainly cover the “inners.” It is not possible to perform this operation so that the outers completely cover the inners. This is not a natural nor desirable outcome.
There are two common operations that are considered labiaplasties: the “trimming” operation (or amputation operation) and the “wedge” operation. Dr. Goldman only performs the wedge operation and explains the differences between these operations at the consultation.
The surgery is performed using traditional surgical techniques but will soon be performed via laser. Laser labiaplasty results in better and potentially faster healing and overall yields better results. The current operation results in scars that are almost imperceptible. The importance of performing laser labiaplasty relates directly to the next topic.
2. Laser Vaginal Canal Rejuvenation
There is now scientific evidence that CO2 (carbon dioxide) laser, through a very specific system, results in the improvement of the vaginal canal lining, including significant tightening. This is so effective in achieving this that it is now being offered as a non-surgical option for women with mild prolapse and certain forms of urinary incontinence. However, the main rejuvenating aspect of this relates to the re-establishment of the glandular structures within the vaginal canal lining.
This is also now being performed after a recent vaginal delivery to prevent undesirable changes in the vaginal canal later in life.
Peri- and post-menopausal women will achieve results in terms of the vaginal canal lining: these women develop a ‘wasting’ of this lining with falling oestrogen levels. This manifests with a condition (in its worst form) called vaginitis.
What happens is the lining layer becomes thin and weak with a resulting loss of vaginal glands. This increases the local trauma but much more importantly, reduces the vaginal lubricating capability, resulting in difficult and painful sex.
Femilift from Alma Lasers or The Mona Lisa Touch from Deka Lasers are the only two systems that can offer this treatment. This is a non-surgical treatment that is often performed in the consulting rooms. It is such a minor procedure that normally, no form of anaesthetic is necessary. 3-4 treatments is usually all that is required.
Dr. Goldman will spend an hour or more with you at the consultation going through your issues and areas of concern. You may only need one or two of the operations but the surgical recommendations will be tailored to your specific needs and requirements.
ABOUT THE AUTHOR
Dr Robert Goldman (FRACS, MB,ChB, B.Sc (hons))
Dr Goldman is a specialist surgeon with a focus on cosmetic surgery. With over 35 years of experience, he has helped thousands of patients in Perth and throughout Australia.
Dr Goldman is a member of FRACS (Fellow of the Royal Australasian College of Surgeons, ID 141033) and has completed advanced training at Royal Perth Hospital WA, Sir Charles Gairdner Hospital and Fremantle Hospital WA.


